A 52-year-old patient presents to the clinic reporting fatigue and shortness of breath while climbing stairs over the past few weeks. The patient also reports swelling in the feet.
During the examination, the patient describes a gradual onset of fatigue and increasing difficulty in performing physical activities, even under light intensity, which is accompanied by swelling in the lower extremities. The patient reports having a sedentary lifestyle because of work. No relevant case of heart failure or sudden cardiac death in the family was reported by the patient. There is no disclosure of any history of diabetes, significant cardiovascular events in the past, smoking, or being overweight.
Clinical Exam
During the clinical examination, the patient presents as fatigued, distressed, with elevated blood pressure at 140/90 mmHg, a heart rate of 92 bpm, a respiratory rate of 19 breaths/min, with normal oxygen saturation of 95%. During examination, the heart sounds include a systolic murmur heard best at the apex of the heart. Peripheral edema is observed bilaterally in the lower extremities of the patient.
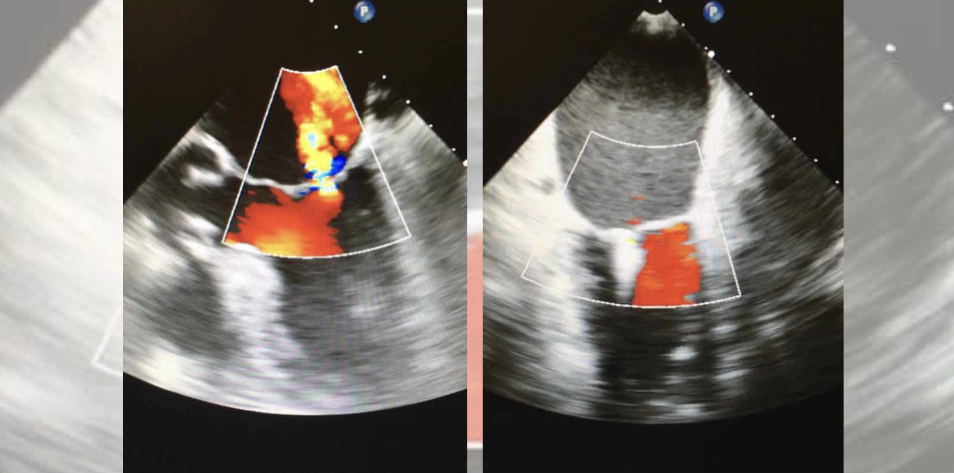
The electrocardiogram reveals normal sinus rhythm and suggestive alterations compatible with left ventricular hypertrophy under resting. A chest X-ray reveals mild pulmonary congestion and ventricular enlargement. The echocardiography (ECG) demonstrates a reduced LVEF of 30% and a moderate mitral valve regurgitation.
Diagnosis
Based on the clinical presentation, ventricular enlargement, decreased LVEF, and echocardiographic findings, the patient is diagnosed with heart failure, which is likely secondary to mitral valve regurgitation. The decreased LVEF correlates with the symptoms of fatigue, dyspnea, and edema experienced by the patient.
Treatment Plan
The treatment plan includes the guideline-recommended pharmacological therapy. Initially prescribed to the patient is a diuretic, associated with an angiotensin-converting enzyme inhibitor, and a beta-blocker. Further examinations with a specialist are recommended to determine the necessity of specific intervention for the valve dysfunction, possibly including a mitral valve repair or replacement.
Besides pharmacological treatment, lifestyle modifications are recommended for this patient’s treatment. It is important to highlight the relevance of dietary changes, reducing sodium intake and ultra-processed, high-caloric foods, and adherence to regular physical activity as tolerated. The adherence to prescribed medications is a fundamental point since many patients frequently do not take the medications correctly. The regular monitoring of symptoms, vital signs, and cardiac function to adjust the management and dosages is a required follow-up need.
Causes of Chronic Mitral Valve Regurgitation
Of note, there are different causes of chronic mitral valve regurgitation. The most frequent primary causes are degenerative mitral valve disease, rheumatic heart disease, and congenital malformations, among others. There are also secondary causes of mitral valve regurgitation, including coronary heart disease with adverse ventricular remodeling, and dilated cardiomyopathy, among others. The extensive use of color flow Doppler echocardiography, a more sensitive method for valvular regurgitation detection, has significantly augmented the detection of this condition.
References
Figure 1 – The future of medical education [Internet]. [cited 2024 Jun 26]. Managing Heart Failure. Available from: https://app.figure1.com/cme/52c8651d-9480-4584-905d-7c8308e2427b
Heidenreich, Paul A., et al. “2022 AHA/ACC/HFSA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines.” Journal of the American College of Cardiology 79.17 (2022): 1757-1780
Lavall, Daniel, et al. “Mitral valve interventions in heart failure.” ESC heart failure 5.4 (2018): 552-561.
Nishimura, Rick A., et al. “Mitral valve disease—current management and future challenges.” The Lancet 387.10025 (2016): 1324-1334.
Published June 26, 2024
Want more clinical cases?
Join Figure 1 for free and start securely collaborating with other verified healthcare professionals on more than 100,000 real-world medical cases just like this one.